
Mammography, Thermography, and Current USPSTF Guidelines for Screening
Mammography, Thermography, and Current USPSTF Guidelines for Screening
By Rick Rydell


EDITOR’S SUMMARY: There’s a reason why every other commercial on YouTube is targeting “Cancer.” In reality, the focus isn’t Cancer at all. As you “read between the lines,” it’s clear the advertiser, Big Pharma, wants to “enlighten” and persuade you to dip further into cure-and-treatment-by-pharmaceuticals. Oh, and watch out for the incredibly long list of health hazards, aka “side effects,” should you dare to enter. Since Big Pharma (big business) and the American Medical Association (AMA) are married, you’re smart to have concerns and doubts when it comes to the push for regular mammogram screenings. Question who has your best interest in mind, dig into the research, and choose with informed consent.
Save the bosom! Think pink! Protect yourself! Since the official advent of breast cancer awareness month nearly 40 years ago, catchy slogans have abounded in pop culture reminding you to make breast cancer prevention a personal priority.
A big part of that prevention: mammography, a technique using X-rays to diagnose and locate tumors in your breasts. Since 1969, modern mammographic tests called mammograms have been squeezing chests in a quest to keep women from dying of breast cancer. Many, if not most, consider it “the gold standard” of breast imaging and cancer prevention.
May 9, 2023: The U.S. Preventive Services Task Force (USPSTF) announces a new draft recommendation stating that all women should receive mammography breast screenings every other year starting at 40 years old.
Previously, the recommendation was that women begin breast imaging at 50 years old, and merely start to have conversations with their practitioners at age 40, to assess when (and if) to begin mammogram screening based on their personal health risks, beliefs, and background history.
Are mammograms all they’re cracked up to be? What about alternatives to mammography, like thermography? Thermography—without touching skin―uses high-tech equipment to measure blood flow patterns, inflammation, and body temperatures to find cancers—a decidedly different approach than boob-smashing mammograms. So what’s the difference? Is one better than the other, and what other options exist?
Mammogram Must-Knows
Breast cancer is a major issue in today’s world. It’s the second-most common cancer for women in the United States behind skin cancer, and American women face a one in eight chance of the dreaded words “breast cancer” being written on their medical charts. Clearly, something is needed to get ahead of the breast cancer epidemic.
Mainstream medicine, including the U.S. Food and Drug Administration (FDA), says that mammogram screenings can help save your life. Here’s what happens during a mammogram. From the University of Texas MD Cancer Center, “Mammograms vs. thermography: What you need to know”:
“During a mammogram, a technologist positions each breast between two plates or paddles. The breast tissue is compressed, and two X-ray images are taken, one from the top and one from the side…
A radiologist studies the images to look for abnormalities. Breast cancer usually appears as a white mass. If your radiologist sees anything abnormal on the mammogram, you’ll be called back for additional imaging.”
If doctors can find tumors in the breast at the earliest stage, the thinking goes, then they can also treat them at the earliest stage. And huge breast cancer organizations like the Susan G. Komen foundation say it works, claiming that mammograms get it right around 87% of the time.
But mammograms are not as simple as taking a blood test, or even undergoing a typical X-ray. They often hurt, plus they can “over diagnose,” or make women undergo treatment like chemotherapy or radiation over breast tissues that turn out to be harmless.
One study noted that although bigger tumors seemed to decrease in incidence after mammography became more widespread (suggesting that mammograms worked in catching cancer early), it was instead primarily the result of the additional detection of small tumors during mammograms. Bigger tumors were no longer making up the highest amounts of breast cancers, it seemed, because so many new smaller tumors were being added to the mix to throw off the numbers.
From the New England Journal of Medicine, in “Breast-Cancer Tumor Size, Overdiagnosis, and Mammography Screening Effectiveness”:
“Women were more likely to have breast cancer that was over-diagnosed [receiving a false-positive diagnosis] than to have earlier detection of a tumor that was destined to become large,” the study’s authors wrote.
Furthermore, “The reduction in breast cancer mortality after the implementation of screening mammography was predominantly the result of improved systemic therapy” for breast cancer like chemotherapy, hormone therapy, and molecularly-targeted therapy."
Some cancer researchers dispute the anointing of mammography as the holy grail of breast cancer prevention and diagnosis. From Medscape Medical News, ‘“Mammography Saves Lives"’ Slogan Doesn't Tell Full Story”:
“The premise of a near universal life-saving benefit from finding pre-symptomatic breast cancer through mammography is false."
Indeed, there is only a 5% chance that a mammogram will save a woman's life, he said, and that percentage must be balanced against potential harms. For instance, when considering women ages 40 to 50:
“[They] are "10 times more likely to experience overdiagnosis and overtreatment than to have their lives saved by mammography.”
One of those potential harms that researchers referenced is radiation. Though the amount of radiation in mammograms is classified as “low dose,” it is still higher than zero. One mammogram, in fact, is comparable to the amount of “natural background radiation” (like exposure to cosmic gas on a flight and radon gas in our homes) we receive on average in seven weeks.
Another downfall: Mammograms give false-positives and false-negatives. While a false-positive may not seem like a big deal (once learning it’s false, that is), and perhaps may be seen as a fortunate second chance at life, a Danish study concluded otherwise.
Annals Of Family Medicine, “Long-Term Psychosocial Consequences of False-Positive Screening Mammography,” found that even three years after being found to be cancer-free, women who had been diagnosed as having breast cancer when they actually didn’t were still reporting negative mental health outcomes like trouble sleeping and feeling anxious.
Another study, from NIH: Population Health Management, “Implications of Overdiagnosis: Impact on Screening Mammography Practices,” estimated that as many as 30% of cancers that undergo treatment like chemotherapy and radiation may not even need it. And the implications of false-negatives are obvious: Women can die for lack of cancer treatment, because they don’t even realize they have it in the first place.
A prime reason for this? Mammograms are limited in their abilities. False-positive results are more common among the following: younger women, those with dense breasts, recipients of breast biopsies, women with relatives who have had breast cancer, or those who are taking estrogen. This means approximately 50% of women who get mammograms over a decade will have a false-positive finding at some point.
Another hard truth: Mammograms may not make much of a difference in the grand scheme of things. One 2009 study concluded that the survival percentage among women ages 50 to 60 who are not screened via mammograms is 99% (although the authors also said that regular mammograms starting at 50 save approximately 1.8 lives over 15 years for every 1000 women screened).
“Understanding the aggressive breast cancers missed by mammogram screening,” a study from Oregon Health & Science University, found that women whose cancer was diagnosed in between mammograms by other methods— meaning that their cancers were missed by mammography—had more lethal tumors.
The tumors that were missed by mammograms were deadlier than the ones spotted by mammography. Such a finding seemingly points to a need for better diagnostics.
A Cochrane review, “Screening for breast cancer with mammography,” seemed to confirm this need. In a review of randomized controlled trials of nearly 600,000 women, scientists found that despite mammograms increasing rates of early breast cancer diagnosis, they failed to reduce the amount of women dying from the disease.
Heatin’ up With Thermography
Thermography, as the name suggests, focuses on temperature differences throughout the body. Though different from high-tech modern machines, the concept has been around for thousands of years; ancient Egyptians spread a thin layer of mud over the sick person’s body and observed the drying rate of different areas.
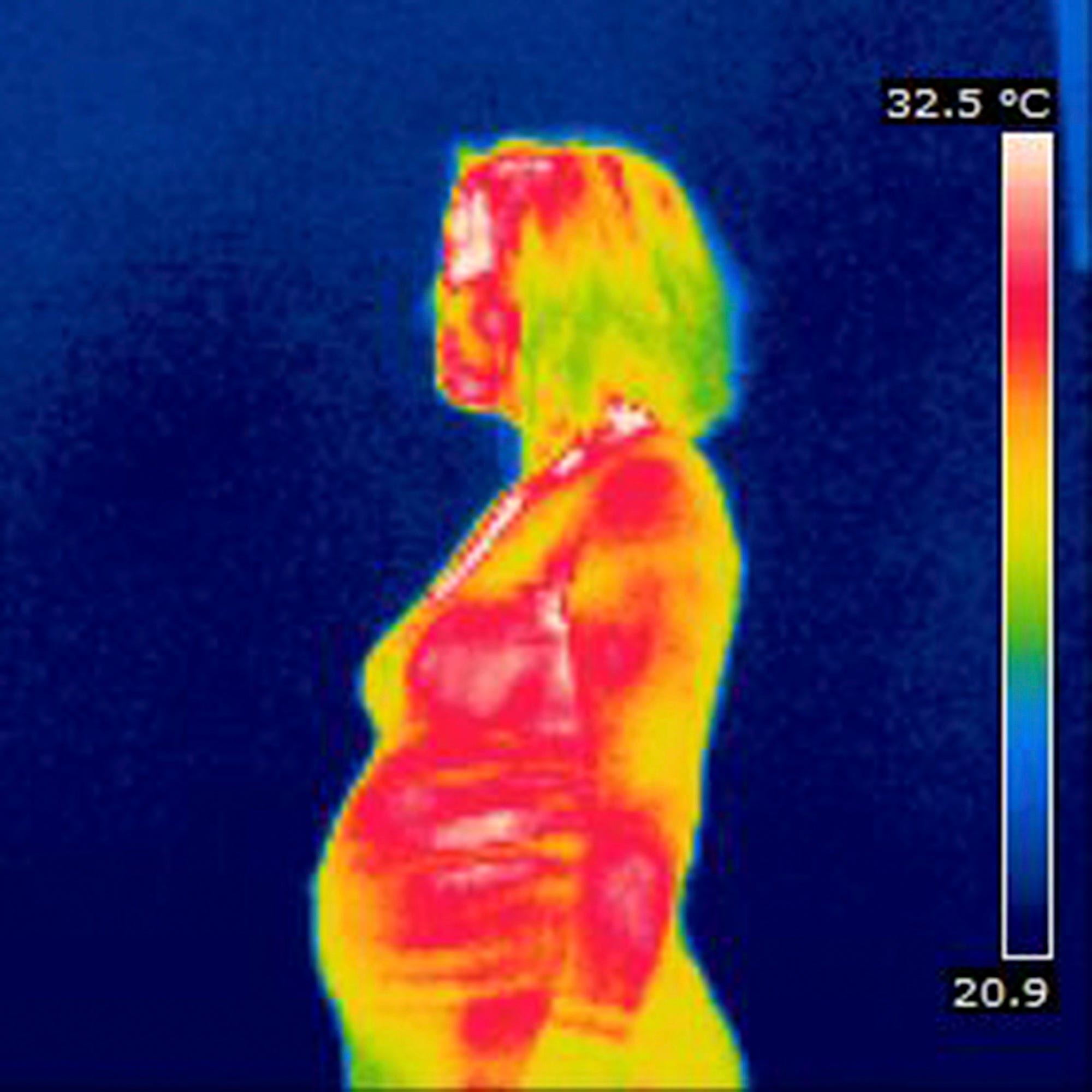
Today’s breast-focused thermography instead uses infrared imaging to measure hotter or cooler areas in the breasts. Since tumors have increased rates of metabolic activity, the logic goes, “hot spots” on a thermogram could theoretically be cancer.
The most tangible benefit: Thermography doesn’t actually touch, or therefore hurt, one of the most sensitive areas of your body—your breasts. It simply scans from a few feet away. It also carries no radiation risk, since it uses digital infrared thermal imaging (DITI) instead. This lack of radiation means that thermography can be used while pregnant and nursing.
Some thermography centers, doctors, and patients claim that thermograms are much better and more accurate for younger and/or denser breasts—the exact kind that mammograms are notoriously bad at diagnosing. The density of breasts simply refers to the appearance of breast tissue on imaging; the less fatty tissue in a breast, the more dense it will show up. About one in ten women have “extremely dense” breasts, meaning that there is almost zero fatty tissue.
The FDA, however, has not published any evidence to support the claims of better accuracy for young and/or denser breasts. Even so, thermograms could theoretically be used for “baseline” body evidence at a much younger age than a normal woman’s first mammogram; most thermographers recommend beginning at age 25.
Therefore, if you have years of thermographic evidence when you hit the breast cancer “danger years” of 40 and beyond, you will most likely be ahead of the game if and when you decide to undergo mammograms or further diagnostic testing of any kind.
Additionally, there are other benefits to thermograms: They can take a look at your armpits, an area that is far harder for mammograms to diagnose. And they may even be able to spot “pre-cancer” areas, since those places often “burn” a little bit brighter on screen (but not as brightly as actual cancer).
The question remains: Are thermograms accurate? Do they actually find breast cancer at rates comparable to mammograms?
A 2016 study, “Comparison of the Accuracy of Thermography and Mammography in the Detection of Breast Cancer,” compared thermograms to mammograms and concluded that the methods are best used in conjunction with each other:
“In the current study, the accuracy of DITI [thermography] was lower than that of mammography (69.7% vs. 76.9%), but the study has some limitations: The sample size is small, and all mass or mass-like densities were examined. In addition, cases fairly inadequate for DITI, such as elderly or morbid obese women, advanced stages of cancer, and large breast sizes, were included in the study.
We believe that DITI is a non-invasive, inexpensive and accessible imaging modality in our country, but its real role in clinical practice could only be evaluated through a large multicenter trial that would estimate the accuracy of digital thermography in breast cancer screening.
At present, our suggestion is to perform thermography as a complementary test to a breast clinical exam. In conclusion, it seems that, despite technical advances in thermography, it cannot substitute for mammography at the present time; this modality can only be proposed as a complementary tool in breast cancer diagnosis.”
Accordingly, the FDA recommends thermography as an “adjunctive” sort of test, meaning it should be used alongside mammography and not solely on its own. It’s worth noting that should a thermographer discover something of concern on your thermogram, they will refer you for further diagnostics—which most likely will include a mammogram.
Most insurance plans, meanwhile, do not cover thermograms as they do with mammograms. Major insurers like Aetna consider the service “experimental and investigational” for breast cancer purposes. That means you’ll likely pay between $150 and $200 out of pocket at a thermography center near you.
Weighing individual risk and circumstances seems to be the clearest move to make in a healthcare area that seems murky. Perhaps “use your brain to make choices about your boobs” would be a wise addition to the canon of catchy breast cancer-related slogans.
Racks and Risks
Just because your doctor tells you to do something, doesn’t mean you have to automatically comply. Take a moment to pause; refrain from accepting tests, drugs, or procedures under duress, fear, or compulsion. When it comes to your body and health, get educated and move at your own pace.
Besides factors like cost and proximity to imaging centers, consider your known personal risk factors for breast cancer when deciding if and when to undergo diagnostic testing:
Age (younger women do not have as high of breast cancer rates)
Breast density (this can usually be diagnosed via breast imaging)
Family history (relatives who have had breast cancer)
Personal health habits (smoking, diet, and exercise)
In addition to traditional mammograms and thermograms, there are other options. For example, digital mammography, which doctors recommend especially if you are under 50, have dense breasts, and/or are still menstruating.
Though these machines are not as widely available as regular mammograms, and cost more, they use a smaller amount of radiation, and their images can be manipulated for better diagnostics.
You might also consider getting an ultrasound, which uses soundwaves to look at the insides of breasts. It can be better for dense breasts, or even to take a further look at something found on a mammogram. Ultrasounds cannot usually detect the earliest signs of breast cancer, however, including tiny calcium deposits called microcalcification. Consider the findings of these cancer researchers.
From the Journal of the Association of Basic Medical Sciences, “Comparative Accuracy Of Mammography And Ultrasound In Women With Breast Symptoms According To Age And Breast Density”:
"Our results indicate that breast density and age are important predictors of the accuracy of mammography. Breast ultrasound is more accurate than mammography in symptomatic women 45 years or younger, mammography has progressive improvement in sensitivity in women 60 years or older.
The accuracy of mammograms increased as women’s breasts became fattier and less dense. In young women and women with dense breasts, ultrasound appears superior to mammography, and may be an appropriate initial imaging test in those women."

Wearing Your Own White Coat
As far as the new guidelines from the USPSTF on jumping into mammographic screening at age 40, you may want to slow down the process. Dr. Vinay Prasad, Hematologist-Oncologist, who has studied and researched Cancer prevention and treatment for over a decade, questions the benefits of screenings, and says the USPSTF “blanket recommendation” is based on “old data.”
From his recent video in "Sensitive Medicine," which goes into depth on mammography analysis, including pros, cons, the “huge overdiagnosis problem,” and real life results, he says:
“You can’t tell someone they live longer; you can’t say you save their life if you have something that in randomized studies have never shown improvement in overall survival. We gotta improve upon that.”
Before considering which road to take, one thing you can do is institute a consistent monthly schedule of zero-risk, non-invasive, no-hassle, self-conducted breast exams. These can also be conducted by your primary health provider or OB/GYN. The worst thing that can happen is that you get to know your breasts very well. And the best? You may get a head start at prevention or early detection, and avoid unnecessary worry or suffering.
~
Originally published by A Voice For Choice Advocacy on May 18, 2023.
If you would like to support the research and health education of AVFC editorial, consider making a donation today.
So much info and food for thought, thank you. I’m 54 and have never had a mammogram. Still on the fence, but not feeling compelled to.